Antibiotics have been one of the crowning achievements of biochemistry in the 20th century – with the golden era of antibiotic discoveries in the 1950-1970s. Their discovery propelled immense advancements in life expectancy and disease management, stopping previously debilitating bacterial infections dead in their tracks. Alas, through a combination of factors in their use and management, and a lack of new antibiotic agents, antibacterial resistance has become a growing concern in global health – one which is only set to grow in severity under current conditions.
Main Mechanisms of Resistance
Resistance chiefly emerges when an antibiotic agent is not delivered in a potent enough dose or form to eliminate the entire population of a bacterium. This allows for some parts of the population to acquire resistance through mutation. Further exposure to the antibiotic provides a selective advantage for the resistant population, which under normal circumstances may have been less evolutionarily fit and unable to compete with the non-resistant populations. The exact biological mechanisms of resistance can be fairly generalized into four broad categories across species and antibiotic agents, mainly:
- – Enzymatic Inactivation:
The bacteria acquire resistance by producing enzymes which interfere or degrade the antibiotic agent. This can be seen with beta-lactamase enzymes which can hydrolyze beta-lactam antibiotics, such as penicillin.
- – Mutations on the Drug Target:
Antibiotic resistance is acquired through modifying the part of the bacterium the drug acts on, thereby rendering the agent obsolete.
- – Efflux Pump Extrusion:
The bacteria express membrane proteins which can remove (extrude) the antibiotic from the bacterial cell, thereby reducing the effect of the agent.
- – Decrease in Antibiotic Uptake:
Bacteria can also alter membrane protein expression to interfere with the entrance of the antibiotic into the bacterial cell, rendering the antibiotic ineffective.
Another particularly important consideration to make is that the resistance mechanisms do not need to be expressed in the population of the target pathogen; they may be expressed by other bacteria of the microbiome of a patient.
The Burden of Resistance
While antibiotic resistance is a concerning phenomenon even in theory, the real world consequences are equally sobering. A comment published in the Lancet estimated that the leading five antibiotic-resistant diseases in Europe were responsible for 670k+ cases in 2015, presenting a similar disease burden to HIV, tuberculosis and influenza combined. Yet the majority of the response to the growing phenomenon of resistance has been healthcare-oriented, focused around improving the use and management of existing antibiotics. This includes using antibiotics only when truly necessary, ensuring high levels of treatment adherence, and other measures most people are already familiar with when taking antibiotics.
Antibacterial Development: A Financial Quandary
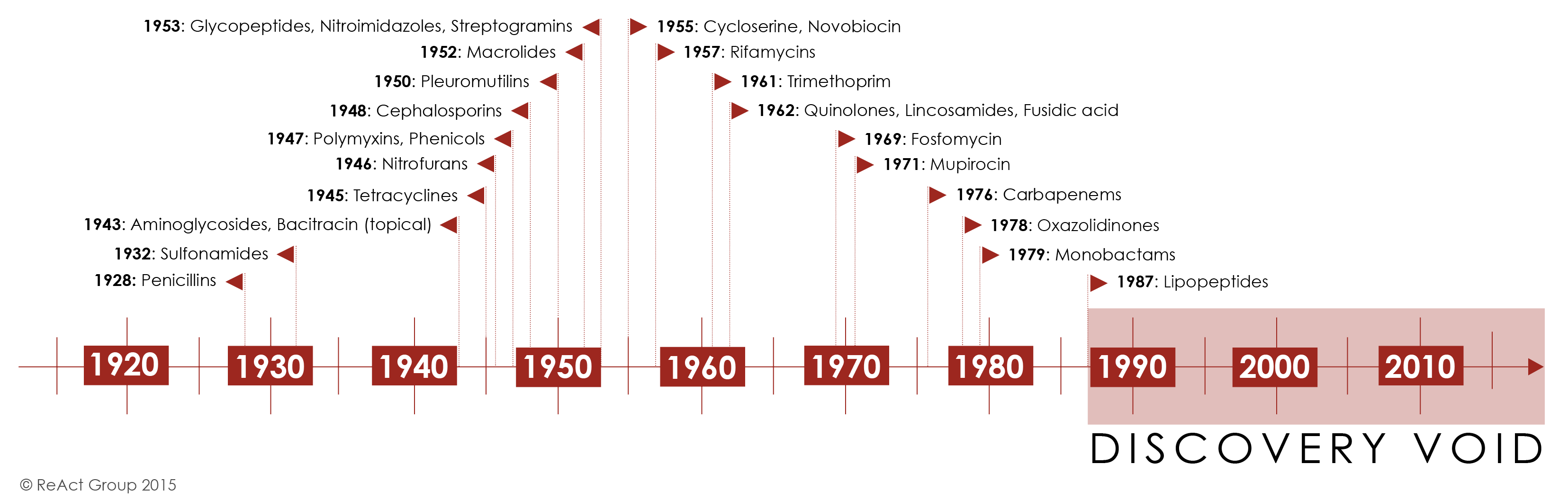
One has to question why this has been the bulk of the response – and one only needs to look at the data for new antibiotics in development over the last three decades to find the answer. The majority of antibiotic classes were pioneered in the 1950s-1970s. After the development of the last two major new classes of antibiotics, with lipopeptides in 1987 and linezolid, the first oxazolidinone, reaching the market in 2000, few new classes of antibiotics have been discovered.
The simple fact is that developing new antibiotics simply does not pose a good return on investment for pharmaceutical companies. Antibiotics are highly effective treatments that only need to be bought for two weeks. The cost of developing an antibiotic is ~$1.5b, while the revenue it generates is estimated to be ~$46m annually; this is insufficient to generate a profit during the exclusivity period of most antibiotics.
Major pharma companies already quit the field in the 2010s, including Sanofi, AstraZeneca, Novartis and others. Exploring new agents can carry significant new side effects as antibiotics can affect the entire microbiome of the human body. This can be accompanied by very unpredictable adverse reactions, particularly for new classes of antibiotics, which pushes the development cost even higher. This quandary was identified early in the 2000s, when the development of novel antibacterial agents was already waning.
Governments and regulators have taken note, and have recently begun steps to ameliorate the issue. This includes plans such as the pilot scheme, organized by the UK government, to provide funds for the development of novel antibiotics on a subscription-based model that would pay for access to any marketed products, rather than paying on a per-pill basis. Sentiment in other countries is also improving.
New Developments
While antibiotics remain expensive to develop – someone will have to pay for that development; whether it be the government or the customer. The other thing to consider would be the reduction in cost to develop – this is particularly true of the drug discovery phase. Improvements in Artificial Intelligence and Machine Learning promise to cut costs and accelerate drug discovery at phenomenal paces. This has already been seen in the field of antibiotics with the recent discovery of Halicin, which was identified to have potent antibacterial activity after a database of 100m compounds was screened in just three days. Halicin shows significant potential through its completely novel mechanism of action, which disrupts electrochemical gradients across bacterial cell membranes by sequestering iron intracellularly. This effect prevents the production of energy and should be a difficult mechanism to evolve resistance to.
Other innovations include the designing of small-molecule scaffolds for the delivery of cellular envelope-targeting antimicrobials, such as the THCz molecule discovered at Karolinksa Institute this year. THCz showed the potential to target multiple components, such as teichoic acid, peptidoglycan, capsule and central lipid carriers – the development of strains resistant to all modes of action would be much harder. Another significant advantage offered by THCz is the ease of synthesis for small-molecule based agents, compared to natural cell wall-interfering antibiotics, which would make exploratory investigations far less costly.
It is clear that antibiotic resistance is a growing concern – but managing the use of our current portfolio of antibiotics will merely slow down the inevitable arrival of further resistance. To stay on top of the antibacterial arms race, we require a constant pipeline of development for new antibiotics. This is perhaps the chief challenge for tackling antibiotic resistance. To overcome these obstacles, we require a re-imagination of the monetization model for the development of antibiotics, as well as improvements in technology that promise to reduce development time and costs. Small steps can be seen in both regards, but far greater progress must be committed.
Nick Zoukas, Former Editor, PharmaFEATURES
Subscribe
to get our
LATEST NEWS
Related Posts

Infectious Diseases & Vaccinology
Enduring Blockade: Five-Year Functional Antibody Persistence Against Emerging GII.4 and GII.17 Noroviruses
Natural infection with dominant GII noroviruses elicits long-lived functional antibodies, redefining immune durability in viral gastroenteritis.
Infectious Diseases & Vaccinology
Resistant Mycosis: Reimagining Antifungal Therapy Through Mechanistic Innovation and Molecular Disruption
Emerging antifungal strategies are redefining treatment by targeting fungal physiology through diversified, mechanism-driven approaches that overcome entrenched drug resistance.
Infectious Diseases & Vaccinology
Fungal Refractory States: Deciphering Pathobiology and Therapeutic Weaknesses in the Era of Rising Antifungal Resistance
Rising antifungal resistance reflects a multidimensional biological challenge that demands mechanistically innovative, host-integrated therapeutic strategies.

Infectious Diseases & Vaccinology
Epigenetic Parasite Vulnerabilities: Repurposing Histone Deacetylase Inhibitors for Complex Multispecies Therapeutics
Repurposed HDAC inhibitors target essential parasite epigenetic machinery, offering a powerful but complex frontier for next-generation antiparasitic therapy.
Read More Articles




Medicinal Chemistry & Pharmacology
February 16, 2026
Spatial Collapse: Pharmacologic Degradation of PDEδ to Disrupt Oncogenic KRAS Membrane Localization
PDEδ degradation disrupts KRAS membrane localization to collapse oncogenic signaling through spatial pharmacology rather than direct enzymatic inhibition.

Medicinal Chemistry & Pharmacology
February 4, 2026
Neumedics’ Integrated Innovation Model: Dr. Mark Nelson on Translating Drug Discovery into API Synthesis
Dr. Mark Nelson of Neumedics outlines how integrating medicinal chemistry with scalable API synthesis from the earliest design stages defines the next evolution of pharmaceutical development.

Clinical Operations
February 3, 2026
Zentalis Pharmaceuticals’ Clinical Strategy Architecture: Dr. Stalder on Data Foresight and Oncology Execution
Dr. Joseph Stalder of Zentalis Pharmaceuticals examines how predictive data integration and disciplined program governance are redefining the future of late-stage oncology development.

Medicinal Chemistry & Pharmacology
February 2, 2026
Exelixis Clinical Bioanalysis Leadership, Translational DMPK Craft, and the Kirkovsky Playbook
Senior Director Dr. Leo Kirkovsky brings a rare cross-modality perspective—spanning physical organic chemistry, clinical assay leadership, and ADC bioanalysis—to show how ADME mastery becomes the decision engine that turns complex drug systems into scalable oncology development programs.

{kind=link}
Regulatory Affairs
January 30, 2026
Policy Ignition: How Institutional Experiments Become Durable Global Evidence for Pharmaceutical Access
Global pharmaceutical access improves when IP, payment, and real-world evidence systems are engineered as interoperable feedback loops rather than isolated reforms.