Hidden within the roots and bark of the common apple tree lies a compound with remarkable therapeutic potential. Phloretin, a naturally occurring dihydrochalcone glycoside, has emerged as a multifaceted agent exhibiting significant anti-inflammatory properties. Originally isolated in the 19th century, phloretin and its glycoside form, phlorizin, have captured the attention of the scientific community for their diverse biological activities. This article delves into the comprehensive understanding of phloretin’s mechanisms of action and its promising role in combating various inflammatory diseases.
The Discovery of Phlorizin and Phloretin
In 1835, phlorizin was first extracted as a bitter-tasting substance from the root bark of the apple tree (Malus domestica). Found predominantly in young shoots, roots, leaves, bark, and seeds, phlorizin can constitute up to 14% of the dry weight of apple leaves, varying with the cultivar. Known by several names—phloridzin, phlorhizin, phlorizoside—this compound laid the groundwork for understanding a class of molecules with significant pharmacological effects.
Phlorizin’s importance extends beyond its natural occurrence; it has been instrumental in the development of selective sodium-glucose cotransporter-2 (SGLT2) inhibitors. These inhibitors, such as dapagliflozin, canagliflozin, and empagliflozin, are now pivotal in the treatment of diabetes mellitus by promoting urinary glucose excretion and aiding in glycemic control.
Structural Significance and Pharmacological Properties
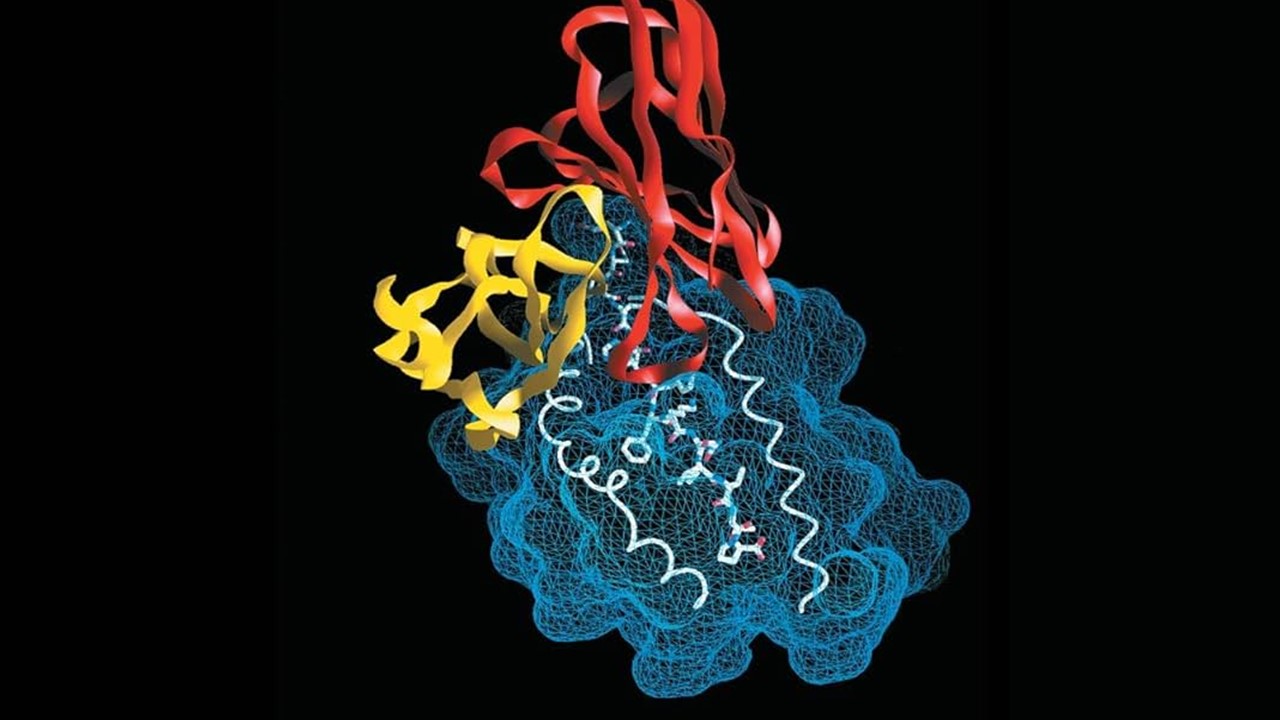
The molecular structure of phlorizin features a glucose moiety linked to a dihydrochalcone backbone, which is crucial for its biological activity. Its aglycone form, phloretin, lacks this glucose component but exhibits its own set of pharmacological effects. While phlorizin is a potent inhibitor of SGLT2 in the nanomolar range, phloretin demonstrates a broader spectrum of activity, albeit with lower potency in glucose transporter inhibition.
One significant limitation of phlorizin as an oral therapeutic agent is its poor bioavailability due to rapid hydrolysis by intestinal β-glucosidases, resulting in the formation of phloretin. This metabolic conversion not only reduces phlorizin’s efficacy but also introduces phloretin into systemic circulation, where it exerts distinct biological effects.
Mechanisms of Action: Targeting Glucose Transporters
Phlorizin’s ability to inhibit SGLT2 and, to a lesser extent, SGLT1, disrupts glucose reabsorption in the kidneys, leading to increased urinary glucose excretion. This action provides a mechanism for glycemic control without inducing hypoglycemia. However, the inhibition of SGLT1 and other glucose transporters can result in undesirable side effects, such as gastrointestinal disturbances and renal impairment.
Phloretin, on the other hand, is known to inhibit glucose transporter 1 (GLUT1) and other facilitative glucose transporters (GLUTs). In immune cells like macrophages, GLUT1 expression is upregulated during activation, enhancing glucose uptake and glycolysis to meet the energy demands of the inflammatory response. By inhibiting GLUT1, phloretin can modulate this metabolic shift, thereby exerting anti-inflammatory effects.
Phloretin’s Anti-Inflammatory Effects on Macrophages and Immune Cells
Macrophages are pivotal players in the initiation and resolution of inflammation. Phloretin has been shown to suppress the activation of macrophages stimulated by lipopolysaccharide (LPS), a component of bacterial cell walls that triggers an immune response. In vitro studies demonstrate that phloretin reduces the production of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6).
The compound achieves this by inhibiting the nuclear factor kappa B (NF-κB) signaling pathway, a critical regulator of inflammatory gene expression. Phloretin prevents the degradation of the inhibitor of kappa B alpha (IκBα), thereby blocking NF-κB translocation to the nucleus and subsequent transcription of pro-inflammatory genes. Additionally, phloretin suppresses the phosphorylation of mitogen-activated protein kinases (MAPKs), including ERK, JNK, and p38, further dampening the inflammatory response.
Beyond macrophages, phloretin affects other immune cells by modulating Toll-like receptor (TLR) signaling. It inhibits TLR2 and TLR4 pathways, which are instrumental in recognizing pathogenic molecules and initiating inflammation. This broad-spectrum modulation of immune cell activation positions phloretin as a promising anti-inflammatory agent.
Modulation of Obesity-Associated Inflammation
Obesity is often accompanied by chronic low-grade inflammation, contributing to metabolic disorders such as insulin resistance and non-alcoholic fatty liver disease (NAFLD). Phloretin has demonstrated the ability to inhibit adipogenesis—the formation of fat cells—and promote lipolysis, thereby reducing lipid accumulation in hepatocytes.
In animal models of high-fat diet-induced obesity, phloretin administration resulted in decreased body weight, reduced liver lipid accumulation, and improved hepatic steatosis. The compound modulates key metabolic regulators, including the activation of AMP-activated protein kinase (AMPK) and upregulation of sirtuin 1 (SIRT1), leading to enhanced fatty acid oxidation and decreased lipogenesis.
Phloretin also exhibits anti-inflammatory effects in adipose tissue by suppressing the expression of pro-inflammatory cytokines and chemokines. It promotes a shift in macrophage polarization from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, reducing adipose tissue inflammation and improving insulin sensitivity.
Protective Roles in Endothelial Inflammation and Injury
Endothelial dysfunction is a hallmark of various cardiovascular diseases and is often exacerbated by hyperglycemia and inflammation. Phloretin has been shown to protect endothelial cells from high glucose-induced injury by reducing the expression of adhesion molecules such as vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule-1 (ICAM-1). This reduction decreases the adhesion of monocytes to the endothelium, a critical step in atherogenesis.
The compound also inhibits the activation of transforming growth factor-beta (TGF-β) and the downstream Smad2 signaling pathway, which are involved in vascular fibrosis. By activating AMPK and enhancing the expression of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α), phloretin mitigates endothelial injury and promotes vascular health.
Furthermore, phloretin’s antioxidant properties contribute to its protective effects. It enhances the activity of antioxidant enzymes like manganese superoxide dismutase (MnSOD) by increasing the expression of SIRT3, thereby reducing oxidative stress in endothelial cells.
Respiratory Benefits: Phloretin in Lung Inflammation
Phloretin’s anti-inflammatory prowess extends to the respiratory system, where it has shown efficacy in models of lung injury and asthma. In lung epithelial cells, phloretin reduces the production of pro-inflammatory mediators such as prostaglandin E2 (PGE2), IL-8, and MCP-1. It achieves this by inhibiting NF-κB activation and MAPK phosphorylation, similar to its mechanisms in macrophages.
In animal models of asthma induced by ovalbumin, phloretin administration decreased airway hyperresponsiveness, eosinophil infiltration, and goblet cell hyperplasia. It also reduced the levels of Th2 cytokines, chemokines, and adhesion molecules in lung tissues, highlighting its potential as a therapeutic agent in allergic airway diseases.
Moreover, phloretin has demonstrated protective effects against lung inflammation induced by cigarette smoke and bacterial infections. By inhibiting the expression of mucin proteins and inflammatory cytokines, it may offer benefits in chronic obstructive pulmonary disease (COPD) and other respiratory conditions.
Potential in Arthritis Treatment
Inflammatory joint diseases like rheumatoid arthritis and osteoarthritis involve the overproduction of pro-inflammatory cytokines and degradative enzymes that destroy cartilage and bone. Phloretin has shown promise in ameliorating these effects by suppressing the expression of COX-2, iNOS, and matrix metalloproteinases (MMPs) in chondrocytes.
In collagen-induced arthritis models, phloretin treatment resulted in reduced joint inflammation, decreased cytokine levels, and protection against cartilage degradation. By inhibiting the PI3K/Akt and NF-κB signaling pathways, phloretin mitigates the inflammatory processes underlying arthritis, offering a potential avenue for therapeutic intervention.
Gut Health: Phloretin’s Role in Intestinal Inflammation
The gastrointestinal tract is susceptible to inflammation from various sources, including pathogens, toxins, and autoimmune reactions. Phloretin has demonstrated significant anti-inflammatory effects in models of ulcerative colitis and bacterial-induced colitis.
By modulating the gut microbiota, phloretin helps restore the balance between beneficial and harmful bacteria, reducing dysbiosis associated with inflammatory bowel diseases. It suppresses the activation of the NOD-like receptor family pyrin domain containing 3 (NLRP3) inflammasome and NF-κB pathway, leading to decreased production of pro-inflammatory cytokines.
Additionally, phloretin enhances the expression of tight junction proteins like zonula occludens-1 (ZO-1) and occludin, strengthening the intestinal barrier and preventing bacterial translocation and further inflammation.
Hepatic and Renal Protective Effects
Phloretin’s anti-inflammatory and antioxidant properties extend to the liver and kidneys, where it offers protection against toxin-induced injury. In models of non-alcoholic fatty liver disease and hepatic fibrosis, phloretin reduces lipid accumulation, oxidative stress, and inflammatory cytokine production.
In the kidneys, phloretin has been shown to alleviate hyperuricemia-induced renal injury by suppressing the expression of GLUT9, reducing uric acid reabsorption, and inhibiting the NLRP3 inflammasome pathway. This leads to decreased inflammation, fibrosis, and improved renal function.
Moreover, phloretin mitigates nephrotoxicity induced by drugs like cisplatin by reducing oxidative stress markers and inflammatory cytokines, highlighting its potential as a renoprotective agent.
Cardioprotective and Neuroprotective Actions
Phloretin exhibits protective effects on the heart and nervous system by targeting inflammation and oxidative stress. In diabetic cardiomyopathy models, it reduces cardiac hypertrophy, fibrosis, and improves myocardial function. By activating the Nrf2 pathway and increasing antioxidant enzyme expression, phloretin combats hyperglycemia-induced oxidative damage in cardiac cells.
In neurodegenerative disease models like Parkinson’s and Alzheimer’s, phloretin enhances cognitive function, decreases neuroinflammation, and reduces neuronal apoptosis. Its ability to suppress microglial activation and pro-inflammatory cytokine production contributes to its neuroprotective effects.
Additionally, phloretin improves diabetic neuropathy symptoms by alleviating hyperalgesia, reducing oxidative stress, and suppressing inflammatory mediators in nervous tissues.
Phloretin in Skin Inflammation and Beyond
The skin, as the body’s largest organ, is subject to various inflammatory conditions such as dermatitis and acne. Phloretin has shown efficacy in reducing skin inflammation by inhibiting the release of histamine, cytokines, and prostaglandins. In models of atopic dermatitis, it suppresses the proliferation of Th1, Th2, and Th17 cells, leading to reduced inflammation and improved skin barrier function.
Phloretin’s antioxidant properties also protect skin cells from ultraviolet-induced damage and oxidative stress, suggesting potential applications in dermatology and anti-aging therapies.
Unveiling the Therapeutic Future of Phloretin
From its origins in apple tree bark to its multifaceted roles in human health, phloretin emerges as a powerful anti-inflammatory agent with broad therapeutic potential. Its ability to modulate key signaling pathways, suppress pro-inflammatory mediators, and protect against oxidative stress positions it as a promising candidate for the treatment of various inflammatory diseases.
Challenges such as poor bioavailability remain, but advancements in formulation techniques and delivery systems hold promise for overcoming these limitations. As research continues to unveil the depth of phloretin’s biological activities, it may soon find its place as a valuable tool in the arsenal against inflammation and its associated pathologies.
Study DOI: https://doi.org/10.3390/biomedicines11010143
Engr. Dex Marco Tiu Guibelondo, B.Sc. Pharm, R.Ph., B.Sc. CpE
Editor-in-Chief, PharmaFEATURES

Subscribe
to get our
LATEST NEWS




Related Posts
Medicinal Chemistry & Pharmacology
Aerogel Pharmaceutics Reimagined: How Chitosan-Based Aerogels and Hybrid Computational Models Are Reshaping Nasal Drug Delivery Systems
Simulating with precision and formulating with insight, the future of pharmacology becomes not just predictive but programmable, one cell at a time.
Medicinal Chemistry & Pharmacology
Coprocessed for Compression: Reengineering Metformin Hydrochloride with Hydroxypropyl Cellulose via Coprecipitation for Direct Compression Enhancement
In manufacturing, minimizing granulation lines, drying tunnels, and multiple milling stages reduces equipment costs, process footprint, and energy consumption.

Medicinal Chemistry & Pharmacology
Decoding Molecular Libraries: Error-Resilient Sequencing Analysis and Multidimensional Pattern Recognition
tagFinder exemplifies the convergence of computational innovation and chemical biology, offering a robust framework to navigate the complexities of DNA-encoded science